Low Dose-what’s the occupancy- Anders Sorensen
How much of your brain’s target receptors are still blocked at “low” doses of antidepressants and antipsychotics? Here’s what receptor occupancy studies show:
•Duloxetine 5 mg → up to 44% of receptors blocked
•Venlafaxine 2.4 mg → up to 34% of receptors blocked
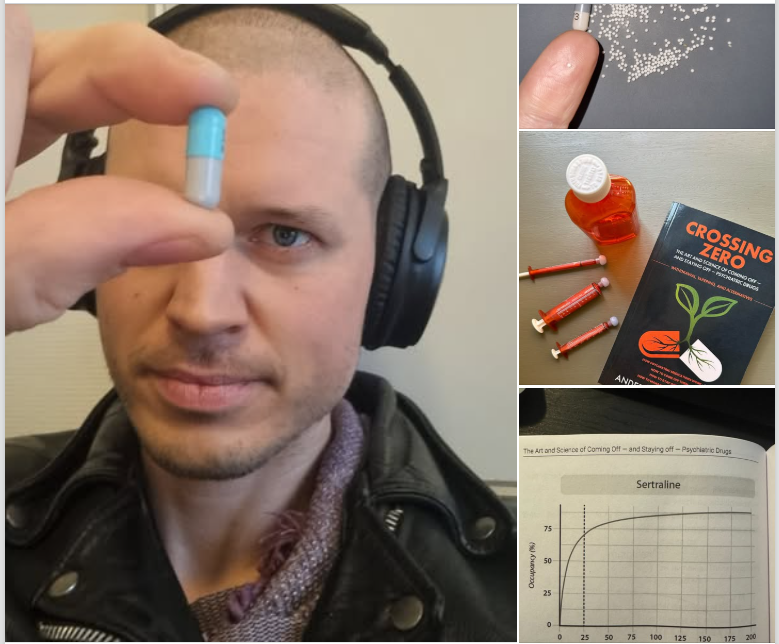
•Sertraline 10 mg → up to 49% of receptors blocked
•Fluoxetine 1 mg → up to 30% of receptors blocked
•Citalopram 1 mg → up to 16% of receptors blocked
•Escitalopram 5 mg → up to 67% of receptors blocked
•Vortioxetine 2.5 mg → up to 49% of receptors blocked
•Paroxetine 5 mg → up to 52% of receptors blocked
•Aripiprazole 1 mg → up to 57% of receptors blocked
•Brexpiprazole 1 mg → up to 64% of receptors blocked
•Olanzapine 2.5 mg → up to 36% of receptors blocked
•Lurasidone 10 mg → up to 43% of receptors blocked
•Risperidone 1 mg → up to 55% of receptors blocked
Even at what most doctors are taught to call “tiny” doses, these medications still have a powerful effect on the brain. This is why psychiatric drugs must be tapered very slowly – especially at the lower end – if severe and protracted withdrawal is to be avoided after long-term use.
Following the drug’s receptor occupancy curve when tapering is called hyperbolic tapering.
To achieve the 3-10% reductions often needed for a safe taper, people find themselves needing to:
1) Cut and weigh tablets using a pill cutter or razor
2) Open capsules and count the hundreds of tiny beads inside
3) Dissolve the tablet in water to and measure out precise doses with a syringe
So, if your doctor says, “Just stop at the lowest dose,” – educate them. Show them this data – it’s hardcore neurobiology.